Case study — Behavioral-health EMR
Couve
An admissions and revenue platform built so a person knows what treatment costs before they say yes.
One click to sign in · no credentials · all data synthetic
The problem
Four tools each knew half the truth about one patient.
Someone says the hardest yes of their life; three weeks later a $12,000 bill nobody warned them about lands. The coordinator never stood a chance — the answer lived in four tools, each of which shipped half of it:
The thesis
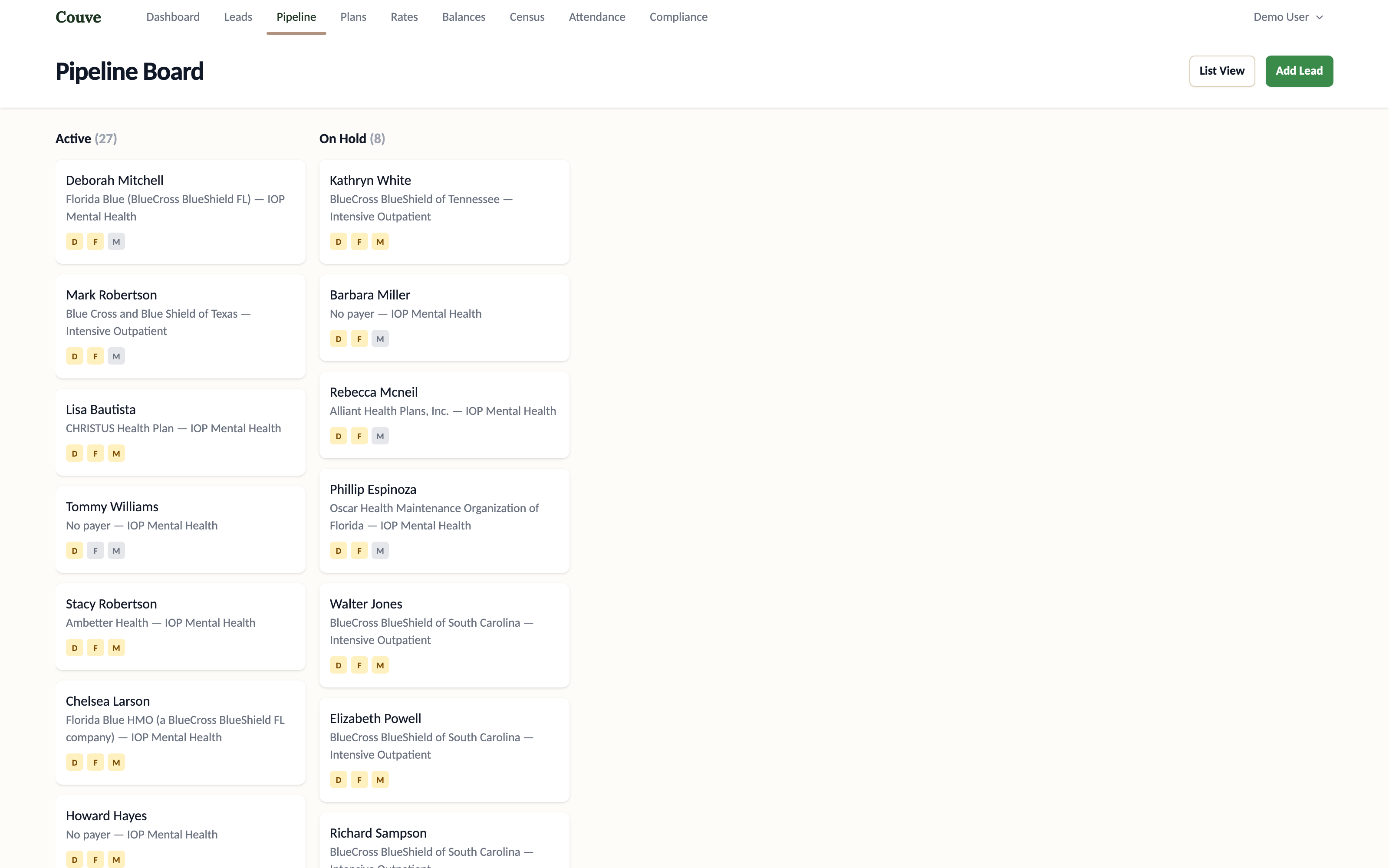
Readiness is one answer, not five systems.
Every admission clears four tracks — demographics, financial, medical, disposition — rolled into one honest state on one patient record. The system’s job isn’t to store records; it’s to say whether this person is ready, and to refuse to pretend when they aren’t.
Admission Readiness
See it run
You’re one click from the coordinator’s chair.
No credentials, no sandbox tour — the demo signs you straight in. Work the pipeline, open a lead, run an estimate, try to admit someone who isn’t cleared. The data is synthetic and resets itself; the behavior is real.
The decisions
Make the money knowable. Make the gates honest.
Nobody says yes to treatment blind.
A real verification of benefits becomes a plain-language, session-by-session estimate priced on the contracted rate. A frightened person can plan around a number; nobody plans around an EOB.
▶ Live — this is math, not a screenshot
Some steps shouldn't be polite suggestions.
You cannot admit someone whose benefits are only “requested” — the system blocks it, in red, with the reason. Deliberate friction, placed exactly where skipping ahead becomes a surprise bill.
Plain language, no billing-code fluency required.
Dispositions, human-readable timelines, contracted rates you can actually see. An EMR is measured by how fast one tired coordinator can find the truth.
No org name is hardcoded anywhere.
Branding, facilities, payers, rates — all configuration. Any provider could stand this up without touching the code, because that discipline started at the first commit.
The machinery
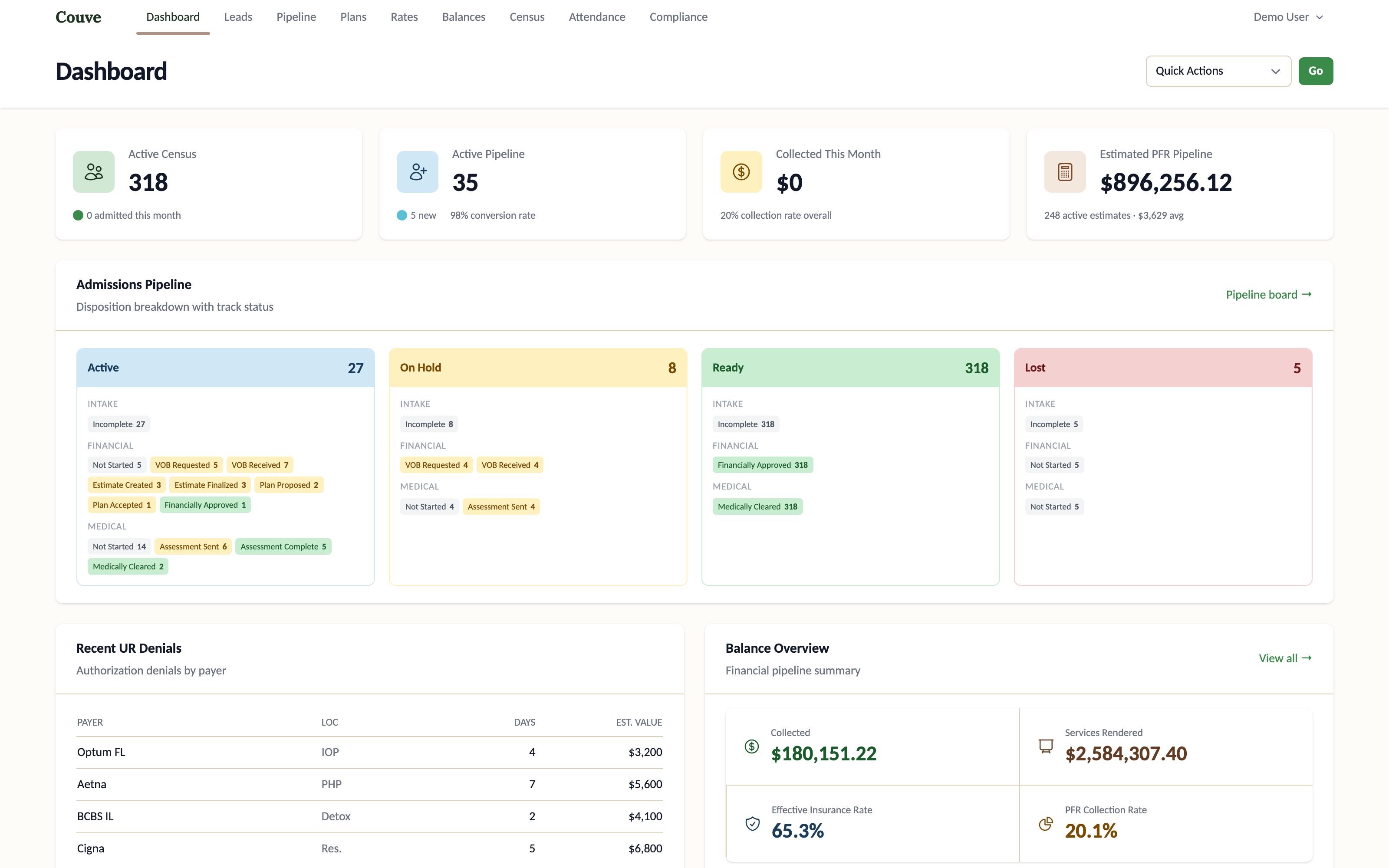
One record, from first call to final payment.
The spine every screen hangs off. Because it’s one record, the dashboard’s revenue pipeline, the readiness gate, and the patient’s estimate can never disagree — they’re reading the same row.
Who did what, plainly
Solo build. Borrowed scars.
I designed and built all of it — schema, workflow, and interface. The judgment inside it isn’t mine alone: it comes from two years working inside a national behavioral-health provider, watching coordinators reconcile these systems by hand. Their workarounds are this product’s requirements.
What a production deployment would add is the load-bearing work a prototype gets to skip: a BAA-backed hosting posture, real payer integrations, and the compliance hardening that protects patients and staff — tracked in the repo as explicit debt, not hand-waved.
Where it landed
Kickoff to a live, seeded demo: five months, solo.
February: first commit. July: a deployed platform with a one-click demo, a 20,000-plan pricing engine, and a seeded operation exercising every readiness state — every claim on this page checkable by clicking around it.
▸ What I’m not claiming: production use, real patients, or measured outcomes — the data is synthetic and no PHI exists anywhere in the system. The claims here are the kind architecture can guarantee, and the demo will show you.
Next
Gab is the front door. Couve is the building.
Every lead here begins as a conversation. Gab, the intake assistant, hands off a lead that arrives demographics-complete — and the moment Couve verifies benefits, the out-of-pocket number can travel back into that conversation. One spine, from a scared 2 a.m. message to an admission with no surprises.